Introduction to Bone Fractures in Different Age Groups
In this article, the Iran Height Increase Center will discuss the differences in bone fractures between children and adults. Although bones in both adults and children are susceptible to fractures, there are differences in the type of fracture, shape, healing process, and other factors that affect the fracturing and healing process in these two groups.

- Introduction to Bone Fractures in Different Age Groups
- Key Differences in Bone Fractures
- Weakness of Periosteum Attachment to Bone in Children
- Distribution of Fracture Incidence
- Healing Process of Fractures
- Progress in Fracture Repair
- Bone Growth After Fracture
- Diagnosis of Fractures
- Need for Surgery in Fractures
- Conclusion and Invitation for Questions
Key Differences in Bone Fractures
1. Presence of Growth Plates
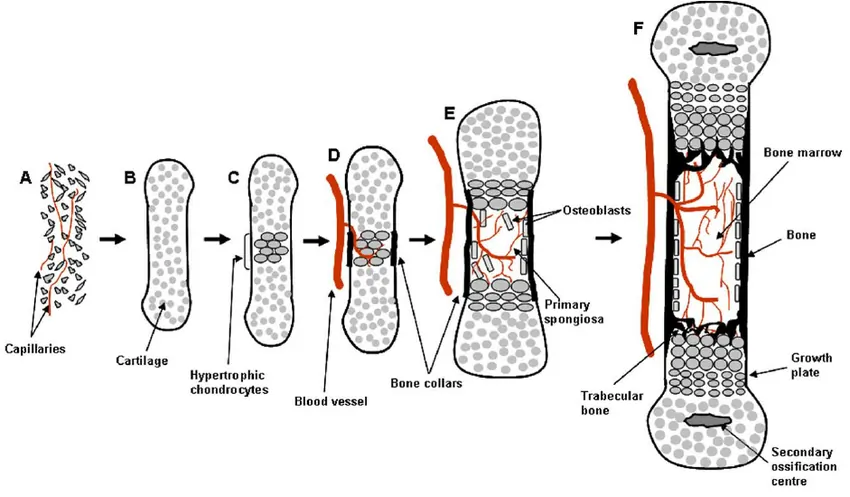
One of the main differences between the bones of children and adults is the presence of growth plates. These cartilaginous plates are usually located at both ends of long bones and are responsible for the longitudinal growth of bones.
Growth plates are weaker areas in bones and are often the first to be damaged in impacts affecting children. Injuries to these plates usually appear as separations from the bone or fracture lines crossing them, known as “growth plate fractures.”
2. Flexibility of Children’s Bones
A significant characteristic of children’s bones is their greater flexibility. When a child’s bone is subjected to impact, it bends like a spring and does not break easily. Children’s bones can withstand greater forces without fracturing, thanks to their flexibility.
Due to this high flexibility, two types of deformations occur in children’s bones after an impact, which are rare in adults. One such type is the “greenstick fracture,” which occurs because of this property of the bone. In this type of fracture, the bone acts like a damp twig on a tree branch under the force, not breaking completely but bending and remaining connected at the site of impact.
Another type of fracture in children is known as “plastic deformation.” In this fracture, the bone bends like a bow along its entire length, and this deformation occurs throughout the bone, resembling the way clay or plastic might bend.
Weakness of Periosteum Attachment to Bone in Children
Periosteum and Its Connection to Bone
The periosteum, or periosteal layer, is a cloth-like layer that covers the bones of the body and is attached to them.
In children, the connection of the periosteum to the diaphysis (the middle region of long bones) is weaker and less stable compared to adults. If the bone fractures, the blood resulting from the fracture quickly accumulates between the periosteum and the bone, separating them.
This blood rapidly turns into a bone callus. Therefore, even in children’s fractures that are non-displaced, a bone callus is present and is larger in size compared to adults.
Distribution of Fracture Incidence
Common Fractures in Children
In children, fractures of the scaphoid and femoral neck are less common. Conversely, fractures in the elbow area are more common in children than adults and are more challenging to treat.
Healing Process of Fractures
Rapid Bone Healing in Children
Bone fractures in children heal faster than in adults, with the highest rate of healing in younger children. In infants, even severe fractures can heal within 2-3 weeks.
This rapid healing rate in children has two significant implications. First, the treatment of children’s fractures must begin swiftly, before the bone starts to heal. Bone fracture treatment in children should start within the first 5 days after the fracture. Second, there is no need for prolonged immobilization of the fractured limb in children, so the duration of cast use is shorter than in adults.

To make an appointment or get an online consultation with Dr. Nader Motallebi Zadeh, Limb lengthening surgeon, proceed here.
Progress in Fracture Repair
Remodeling Capability in Children
The capability for bone remodeling in children is much better, more extensive, and stronger than in adults. Remodeling refers to the body’s ability to gradually return a fractured bone to its original shape before the fracture. However, the bone’s shape might not be exactly as it was before the fracture.
The remodeling capability is greater in fractures near a joint but is less in intra-articular fractures. It is also more limited in correcting improper rotation of broken pieces relative to each other but is greater when these pieces are joined or compressed. The younger the child, the greater the remodeling capability in their bones.
Bone Growth After Fracture
Stimulation of Bone Growth Post-Fracture
Fractures in children can lead to stimulated and accelerated bone growth. This phenomenon is due to increased blood flow to the growth plate as a result of the fracture, subsequently increasing the activity of the growth plate.
However, the length increase caused by this phenomenon is generally minor and often negligible, meaning that the increase in bone size is usually limited. In this process, fractures can also lead to defects or even cessation of bone growth.
If the growth plate is completely destroyed during a fracture, bone growth in that area stops entirely. In such cases, the younger the child, the greater the length discrepancy of the affected part compared to the healthy part at maturity. This is particularly true in cases where part of the growth plate is damaged, and the other remains intact. In these situations, the bone deviates towards the defective side.
Diagnosis of Fractures
Challenges in Diagnosing Fractures in Children
Diagnosing fractures in children can sometimes be very challenging. These fractures are more often seen in cases without displacement or with minimal displacement. In such situations, deformation of the limb, movement of parts, or bleeding are usually not observed.
In younger children, communication can be difficult, and sometimes, due to their crying, assessing their condition can be very challenging. Often in these cases, the history of trauma or parents’ explanations are not effective for diagnosis. Sometimes, parents may even conceal the truth about a child’s injury (if the child has been seriously injured).
Sometimes, diagnosing fractures through observing fracture lines in radiographic images can be very difficult, and in some cases, growth plates may be mistakenly identified as fractures.
A large amount of callus may form after fractures in children, which could be mistakenly diagnosed as a bone infection or even a bone tumor. Consequently, whenever a child cannot move a limb or its function is reduced, the possibility of a fracture in that area must be seriously considered.
Complications of Fractures
Differences in Complications Between Children and Adults
Complications from fractures in children may differ from those in adults. Non-union of fractures is less common in children than in adults, except for fractures of the lateral condyle in the elbow region. In children’s fractures, two primary complications exist.
One of these is damage to the brachial artery in elbow fractures, and the other is ectopic bone formation in callus or fractures in the elbow area. Movement restriction and joint stiffness after fractures are less common in children than in adults.
Need for Surgery in Fractures
Rare Surgical Interventions in Children’s Fractures
Fractures in children rarely require surgery. Most such fractures can be managed with reduction and the use of a cast.
However, there are exceptions, such as fractures of the lateral condyle of the humerus or femoral neck fractures in children, which often require surgical intervention.
Conclusion and Invitation for Questions
Thank you for reading the article on the differences in bone fractures between children and adults. Please feel free to share your questions with us in this area.
To make an appointment or get an online consultation with Dr. Nader Motallebi Zadeh, Limb lengthening surgeon, proceed here.