Introduction to Supracondylar Elbow Fractures in Children: Supracondylar fractures of the elbow in children are among the common types of fractures and constitute about ten percent of all fractures in children. These fractures typically occur due to a child falling.
- How the Fracture Occurs
- Anatomy of the Elbow Joint
- Supracondylar Elbow Fractures in Children
- Symptoms of Supracondylar Elbow Fractures in Children
- Treatment of Supracondylar Elbow Fractures in Children
- Outcomes of Treatment for Supracondylar Elbow Fractures in Children
- Vascular Complications of Supracondylar Fractures in Children's Elbows
- Importance of Vascular and Neurological Examinations After Fracture
- Symptoms of Arterial Injury After Fracture
- Treatment of Arterial Injuries
- Complications of Supracondylar Fractures in Children's Elbows
How the Fracture Occurs
When falling, children instinctively extend their hands forward. The impact of the palm hitting the ground transfers force to the hand and then to the elbow area, causing a fracture.
Anatomy of the Elbow Joint
The elbow joint is composed of three bones: the humerus (upper arm bone) above, and two forearm bones, namely the ulna (lower arm bone) on the side of the little finger, and the radius (upper arm bone) on the thumb side. The ulna is located on the little finger side, and the radius is on the thumb side. The elbow joint functions as a hinge and moves only in one direction.
Supracondylar Elbow Fractures in Children
A supracondylar fracture is located at the lower part of the humerus and above the elbow joint. This type of fracture is the most common elbow fracture in children and is mostly seen in children under 8 years of age.
Due to the risk of vascular injury, this fracture is considered one of the most dangerous elbow joint fractures. The fracture usually occurs when a child falls with the palm hitting the ground.
If a child falls on the palm, the lower part of the bone moves backward, which is called an Extension type fracture. Conversely, if a child falls on the elbow, the lower part moves forward, and this type is known as a Flexion fracture.
For more information on supracondylar elbow fractures in children, continue following the article.
Symptoms of Supracondylar Elbow Fractures in Children
Severe Pain in the Elbow Area
One of the primary indications of this fracture is severe pain in the elbow area. This pain intensifies with the movement of the elbow or when pressure is applied to the fracture site. Pressure on the elbow may lead to a change in the position of the broken pieces and create a crepitus sound (the sound of bones grinding).
Deformation and Swelling of the Elbow
Following the fracture, the shape of the elbow changes and swells within a few hours. Bruising in the skin around the elbow area is another sign of this fracture.
Assessment of Potential Vascular and Nerve Damage
Due to the high probability of vascular and nerve injuries, the treating physician meticulously examines the blood supply and neurological function of the limb and records the findings in the patient’s file.
The Need for Immediate Medical Attention
If a child feels pain in the elbow area after a fall and is unable to straighten the elbow, immediate medical attention is required.
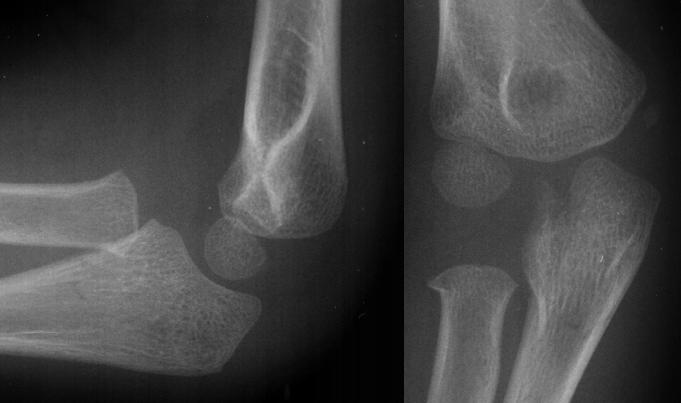
Definitive Diagnosis of the Fracture
The definitive diagnosis of supracondylar elbow fractures is usually made using radiography and imaging of the elbow area.
Treatment of Supracondylar Elbow Fractures in Children
Determining the Type of Treatment
The decision for the type of treatment depends on the extent and direction of the displacement of the broken pieces.
Non-Surgical Treatment
If the fracture is without displacement or with minimal displacement, treatment includes using a splint for the entire upper limb for 3 weeks. During this period, the doctor ensures that no further displacement occurs through repeated imaging of the fracture site.
Surgical Treatment
In the case of displaced fragments, the surgeon performs reduction in the operating room under anesthesia. If the reduction is successful, the limb is immobilized using a splint. Sometimes, the doctor inserts pins through the skin using fluoroscopy to keep the broken pieces in place. If the reduction is not successful, an open reduction is performed, and pins are used to stabilize the fragments. After surgery, the limb is placed in a long splint.
Post-Treatment Measures
After any type of treatment, whether surgical or non-surgical, the elbow should be kept elevated above heart level for a few days to prevent further swelling. The pins are usually removed after 3 weeks, and then elbow movements are initiated to regain range of motion. In the first few days after treatment, careful monitoring of the limb’s blood supply is crucial.
Attention to the Possibility of Vascular Injury
In these types of fractures, there is a high probability of injury to the brachial artery. If it occurs, it must be diagnosed quickly to prevent further damage to the limb.
For more information on supracondylar elbow fractures in children, continue following the article.

To make an appointment or get an online consultation with Dr. Nader Motallebi Zadeh, Limb lengthening surgeon, proceed here.
Outcomes of Treatment for Supracondylar Elbow Fractures in Children
Restoration to Normal Condition After Appropriate Treatment
If the fractured pieces are correctly aligned, the elbow is immobilized for the necessary duration, and the necessary movements for regaining the range of motion are performed after treatment, the elbow usually returns to its normal shape and function. Otherwise, the elbow may become deformed, and its movements may be limited.
Vascular Complications of Supracondylar Fractures in Children’s Elbows
Arterial Injury
In the case of displaced fractures, the sharp edge of the upper fragment can press on the brachial artery, reducing blood flow to the forearm and hand. Sometimes, damage to the inner wall of the artery can lead to clot formation and blockage of the arterial channel. In severe cases, this injury can lead to gangrene or blackening of the fingers.
In most cases, blood reaches the forearm and hand through auxiliary vessels, but this limited blood supply causes changes in the muscles and nerves of the forearm. Muscles gradually get replaced by fibrous tissue, leading to Volkmann’s contracture, where the wrist remains in a bent position. Additionally, reduced blood supply can lead to nerve damage, resulting in decreased or lost sensation in the forearm and hand. These nerve injuries are sometimes reversible and sometimes permanent.
Importance of Vascular and Neurological Examinations After Fracture
In the first few days after the fracture, vascular and neurological examinations and hand movement assessments should be frequently performed. If the above injuries occur, immediate therapeutic actions should be taken to prevent further damage to the muscles and nerves.
Symptoms of Arterial Injury After Fracture
Compartment Syndrome Symptoms
Injury to the brachial artery can lead to compartment syndrome in the forearm. The main sign of this injury is pain along the entire length of the forearm, which worsens with wrist and finger movements. The arterial pulse in the wrist may be absent. Changes in capillary refill, pallor of the hand, decreased sensation or tingling, and paralysis of the hand muscles are other signs of arterial injury.
Treatment of Arterial Injuries
Initial Measures
As soon as arterial injury is diagnosed, emergency treatment must begin. First, any bandage or splint causing pressure on the limb should be removed. If the fracture is displaced and not yet reduced, this must be done quickly to relieve pressure on the artery.
Surgical Interventions
If initial measures are ineffective in improving blood supply, surgery is necessary. In surgery, the brachial artery is exposed, and pressures are relieved. In cases of severe damage, the damaged portion of the artery is replaced with a vascular graft. The fascia around the forearm muscles is also opened to improve blood supply.
Treatment of Volkmann’s Contracture
If damage progresses to Volkmann’s contracture, the changes are often irreversible. However, surgical measures, such as lengthening of the shortened muscles or replacing the damaged muscles with healthy ones, can improve hand function. In severe cases, the wrist joint is fixed in an anatomically acceptable position. If there is serious damage to the median nerve, nerve grafting may help in recovery.
Complications of Supracondylar Fractures in Children’s Elbows
Nerve Damage
There is a possibility of damage to the median and radial nerves in extension-type supracondylar elbow fractures (where the lower fragment is displaced backward) and to the ulnar nerve in flexion-type fractures (where the broken piece is displaced forward).
Median Nerve Injury
The median nerve passes in front of the elbow and may be injured in extension-type fractures. Most of these injuries are reversible and usually recover within a few weeks to months.
Malunion of Fracture
The most common type of malunion is the angulation of the lower fragment inward (cubitus varus). This deformity can cause the forearm to deviate inward and may require surgery if it becomes severe. In surgery, the malunited bone is broken again and positioned correctly.
Heterotopic Ossification
Heterotopic ossification is also a significant complication of supracondylar elbow fractures in children, which can lead to movement limitations of the elbow.
To make an appointment or get an online consultation with Dr. Nader Motallebi Zadeh, Limb lengthening surgeon, proceed here.
Thank you for reading our article on supracondylar elbow fractures in children. Please share your thoughts about supracondylar elbow fractures in children.