What is Blount disease?
Blount disease is a condition in which one growth plate of the upper shin bone grows more slowly than the other growth plate, resulting in a gradual bending of the legs. The illness is typically caused by a diseased growth plate and is progressive, meaning that the child’s bending increases as he or she develops.

Blount disease is more prevalent in overweight and early-walker children. It is also more prevalent among females, African-American and Hispanic children. It may be due to overuse of the inside aspect of the knee. Often mistaken with “physiological bowing,” which develops at a younger age and consists of moderate, symmetrical bowing that resolves on its own. Blount disease, on the other hand, is typically diagnosed between the ages of 2 and 3 and is characterized by an asymmetric, more severe bending of the legs that worsens over time.
Typically, children with scoliosis do not experience any symptoms, although worried parents frequently observe their children’s abnormal gait and crooked legs.
What are the different types of Blount disease?
- Childhood Blount Disease
- This variant of Blount disease affects children under the age of four. It is bilateral (affecting both legs) fifty percent of the time. For treatment to be most effective, it must be administered between ages 3 and 12 and 4 years.
- Teenage Blount Disease
- This kind of Blount disease affects children older than 10 years, particularly those who are overweight. It is less frequent, frequently milder, and more likely to be unilateral (in one leg).
How is Blount disease diagnosed?
The doctor checks a child, watches the child’s gait, and evaluates the rotation and angular look of the leg in order to make a diagnosis. For the identification of the diseased growth plate in the upper tibia and the measurement of the aberrant angulation of the leg bones, an X-ray is necessary.
treatment options for Blount disease
Braces are utilized in non-operative treatment to deload the overloaded inner aspect of the knee. This approach is utilized for mild instances in children younger than 3 years old. Bracing might take up to two years and be difficult.
There are numerous surgical therapies available:
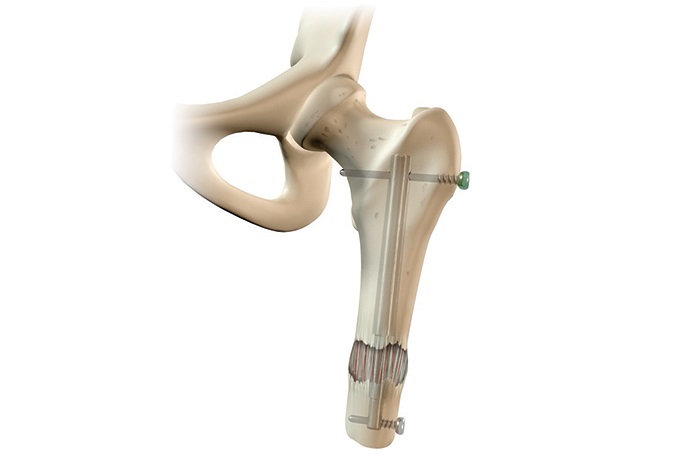
- Corrective osteotomy: The bone is cut and the angulation is corrected. Metal wires are usually used to stabilize the cut bone and the patient is put in a plaster cast usually for 5 to 6 weeks. Alternatively, an external fixator may be used to hold the bones in the corrected position while they heal.
- Guided growth: The healthy side of the growth plate is restricted by using a small plate and two screws, allowing the slow part to make up for the bow and straighten the leg again. This surgery is simple, and the growth arrest of the growth plate is reversible simply by removing the screws. In cases of rebound, the screws are put in again for correction. The surgery takes about 30 minutes and the child can walk immediately after surgery. The period of treatment depends on the amount of correction needed. The patient usually follows up every 4 months to monitor the gradual correction and the screws are removed when the legs are straightened out.
- Hemiplateau elevation: In severe cases where part of the joint line is depressed, the depressed part is elevated through a bone cut. Screws, metal wires, or an external fixator are usually used to maintain correction until bone healing occurs in 5 to 6 weeks. During this time, the child wears a cast and cannot put weight on the leg.
- External fixation: When there is a severe deformity, and especially when the leg is too short, external fixation is commonly used for treatment. The fixator is typically worn on the leg for 3 to 4 months.